Health care workforce diversity is a critical determinant of health equity and the social mission of medical education. Medical schools have a social contract with the public, which provides significant financial support to academic medical centers. Although a focus on diversity is critical in the admissions process for health professions schools, most US medical schools have failed to achieve racial-ethnic or economic diversity representative of the general US population. This article discusses limitations of holistic admissions, structural challenges for diverse learners in medical education, and how to implement socially accountable admissions.
Increasing access to health care, establishing a foundation of cultural humility, and furthering systems-level changes are all needed to address health disparities in our country. Health care workforce diversity is another critical determinant of health equity. Black, Hispanic or Latinx, and Native American health professionals are more likely to practice in underserved communities 1,2 —an important factor in improving access, given that 83 million people in the United States live in health professional shortage areas. 3 Student and faculty diversity, as well as positive interracial interactions, increases medical students’ self-rated cultural competence and decreases their implicit bias. 4,5 A more diverse health care workforce—along with a culture of equity and inclusion—also brings the diversity of perspective, experience, and expertise needed to address the pervasive problem of structural racism in health care and, with it, health inequities. Although the responsibility to diversify the workforce is shared by all schools, it has been effectively accomplished only by a subset of schools, including historically Black colleges and universities and a few public institutions that truly embrace this mandate. 6,7
This mandate is part of each school’s social mission, or the contribution of an institution’s programs, graduates, faculty, and leadership in addressing the health disparities of society. 8 When US medical schools are evaluated using a social mission metric (eg, the percentage of graduates from racial and ethnic groups underrepresented in medicine [URiM] or who are working in health professional shortage areas or practicing primary care), most of those ranked highly by US News and World Report (USNWR) and in terms of National Institutes of Health funding are in the bottom quartile. 7 Over the past 2 decades, as US medical school enrollment has expanded and the population has become more diverse, the percentage of entering medical students from URiM groups, a key metric of social mission, has fallen from 15% to 13%. 9 Even in the most diverse states, the physician workforce does not adequately reflect the population. 10 This lack of representative diversity is itself a product of structural racism and of the culture and systems that perpetuate racial inequality. It is also fundamentally an inequity of economic opportunity. In 2017, 51% of entering US medical students came from the upper quintile of parental income and just 5% from the lowest quintile, 11 revealing a striking economic disparity that has not changed significantly for decades. 12 The health care professions that struggle most with diversity are higher-income professions (eg, physicians, dentists, advance practice clinicians). 13
Health professions education institutions have an overarching social and ethical responsibility to both help dismantle the systems that perpetuate racism and advance policies that will right past wrongs, particularly in their local communities. To become socially accountable, health professions schools will need to change multiple facets of their institutions: their investments in pathway programs and community engagement; their curricula, culture, faculty, and leadership; the metrics they use to predict and ultimately evaluate student success; and their lack of attention to how diversity affects health outcomes. However, the admissions process remains the gatekeeper of access to the profession. In this article, we discuss the limitations of holistic admissions, the challenging environment of medical education for diverse learners, and tools for implementing socially accountable admissions processes, which lay a critical foundation for achieving health professions diversity.
National calls for increasing diversity in medicine are not new, 14,15,16,17,18,19,20 which raises the question: Why haven’t we made more progress? In 2010, the Association of American Medical Colleges (AAMC) established “holistic” review practices to help medical schools make fundamental changes to their admissions criteria, align those criteria with institutional mission and goals, and realize the benefits of diversity. 21 Holistic review requires consideration of how each applicant might contribute value as a medical student and future physician by attaching value to lived experience (E) and personal attributes (A) apart from traditional metrics (M), such as grades and Medical College Admissions Test ® (MCAT) scores. The EAM framework is flexible and seeks to support each institution’s mission, particularly as it pertains to diversity and inclusion. However, there is wide variation in its implementation and little accountability for outcomes. Scores on the MCAT—a convenient and psychometrically sound instrument 22,23 —are influenced by a host of structural influences, including limited academic opportunities and resources reaching as far back as elementary school for students from minority communities. 24 Unfortunately, MCAT scores continue to play a key role in medical school admissions decisions, effectively keeping many students of color from becoming physicians, 6 despite little evidence that such scores predict clinical performance beyond a weak-to-moderate association with scores on other multiple-choice examinations—namely, the steps of the US Medical Licensing Examination ® . 25 MCAT scores also remain part of the influential USNWR rankings, creating an additional incentive for schools to continue to place outsize importance on such scores despite their limited predictive value for important workforce or social outcomes.
Attaching greater value to an applicant’s attributes and experiences, the other 2 components of the AAMC’s holistic (EAM) rubric, makes intuitive sense; the problem is how to operationalize this strategy. Considering personal attributes, such as race and ethnicity—factors we know correlate with important workforce outcomes 1,2 —is prohibited by anti-affirmative action statutes in several states, including California, Texas, and Washington. 26 Even in states without such laws, the threat of being sued is likely “chilling” efforts to change admissions diversity criteria. 27,28 Evaluating applicants’ experiences can also be quite challenging, especially when access to advising, research, and clinical health care experiences is limited by structural and environmental influences, as the COVID-19 pandemic has dramatically illustrated. Access to opportunities is often just the beginning; many URiM learners need to juggle work or family responsibilities with academics. 29 In effect, the deck is stacked against them. To be successful, these students need time, resources, and access to academic development opportunities. How can schools possibly evaluate these learners holistically without accepting these challenges as part of their narrative?
Once admitted to medical school, URiM learners enter less supportive social environments and less positive learning environments and are subject to discrimination and racial harassment at higher rates than their counterparts. 30 Most medical schools sorely lack sufficient minority faculty representation. 31 Faculty members influence the learning experience of all students, but, for minority students, educators who affirm their individuality and values might make the difference between success and failure. 32 Faculty with shared lived experience and understanding of the structural barriers faced by URiM students are more likely to provide the compassion and support needed for these students to succeed. The medical education environment is also rife with grading disparities 33,34,35 and lack of access to professional opportunities, including awards and honors, 36 leading to underdevelopment of URiM learners. In the clinical environment, these students not only witness systemic racism but also may unwittingly participate in it or need to remain silent to avoid putting a grade in jeopardy, again shouldering their community’s disproportionate burdens.
Educators who affirm minority students’ individuality and values might make the difference between success and failure.
Like minority faculty, 37 underrepresented students face additional “taxes” in medical education. 38 While frequently given opportunities to serve on committees, diverse learners are burdened by a disproportionate responsibility to improve the institutional climate and fix the broken system that adversely affects them. They shoulder greater financial stress, feelings of not belonging, microaggressions, stereotype threat, and absence of faculty mentors. Lack of underrepresented faculty likely has an even more profound effect on patient care for communities of color. 39 Unfortunately, the investment and disruption required to nurture and retain learners from marginalized communities may discourage institutions from making necessary structural changes to the learning environment. Bluntly speaking, continuing to educate the economically privileged is easier and cheaper, at least in the short term.
Social accountability refers to the obligation of medical schools to direct their education, research, and service activities toward addressing the priority health concerns of the community, region, or nation they have a mandate to serve. 40 US medical schools have a social contract with the public, which provides significant financial support to academic medical centers for education and training. States provide direct funding to public medical schools, and the federal government provides student loans, grants for education and research, and graduate medical education support to teaching hospitals. 41 To produce the health care professionals and medical researchers that society needs, medical schools must change admissions practices, particularly the emphasis on metrics such as the MCAT and USNWR rankings.
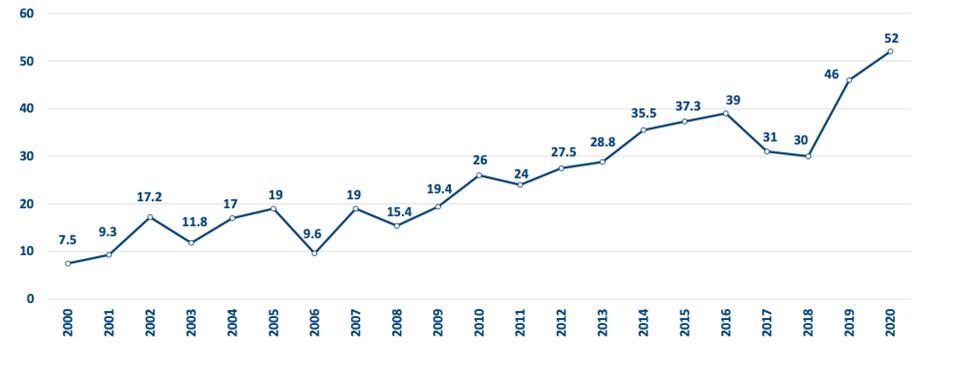
In 2006, the University of California Davis School of Medicine (UC Davis) began implementing a series of structural changes to admissions to enhance diversity and better meet its social mission, resulting in progressive increases in enrollment of URiM students and better representation of California’s population (see Figure). These changes included having admissions personnel participate in the AAMC holistic admissions workshop, appointing new associate and assistant deans of admission, implementing multiple mini-interviews, enhancing diversity of admissions personnel, actively involving students in the admissions process, and developing an admissions mission statement that committed to matriculating a class of future physicians who would address the diverse health care workforce needs of the region. UC Davis also developed a socioeconomic disadvantage score, 42 which systematically attaches value to lived experiences of economic or educational disadvantage, shifting admissions criteria away from grade point average and MCAT scores to a proxy for grit, resilience, and perseverance. More generally, schools’ emphasis on alternative metrics, including multiple mini-interviews and other socially conscious criteria, might result in greater economic and racial-ethnic diversity among medical students. 42,43 In 2020, 35% of entering UC Davis medical students qualified for the AAMC Fee Assistance Program, 44 reflecting significant financial need, compared to 13% of the general pool of US applicants.
Figure. Percentage of UC Davis School of Medicine Matriculants From URiM Groups, 2000-2020 a
a Data from UC Davis School of Medicine Admissions Office records; race/ethnicity tabulated from American Medical Colleges Application Service applications. URiM groups include students who identify as American Indian/Alaskan Native, Black/African American, Hispanic/Latinx, Native Hawaiian, or Filipino.
With a mission that explicitly prioritizes needs of the community, institutions can then partner with those communities to cultivate the next generation of clinicians. By working with local community colleges and academic enhancement programs, 45 providing funding for community-based prehealth initiatives, and bridging otherwise siloed pathway programs, several institutions are attempting to cultivate “hometown” physicians who are likely to return to serve their communities. 9,46,47,48 Other successful strategies for addressing health workforce shortages include selecting students from communities that have the greatest health needs 49,50 ; locating programs in or near the communities they serve, 51 particularly in primary care settings; integrating social determinants of health into the curriculum; and emphasizing a commitment to public service and social accountability across the institution. 52
Ultimately, social accountability must be an institutional priority or mission area in addition to education, research, and clinical care. While policies related to an inclusive campus climate are ubiquitous, accountability is lacking. On the road to social accountability, we must start with soul searching, going beyond course evaluations and learner surveys to critically examine health outcomes and equity measures within our institutions, including how diverse learners and physicians affect patient care outcomes. We must share these outcome measures transparently with community partners and work on solutions together. We must also make investments in financial aid, scholarships, faculty development, antiracism training, and robust community partnerships. As a medical community, we must commit to empowering, supporting, and retaining diverse learners to become future leaders in health care and equity champions.
While calls for increasing representation in medicine are nearly universal, medical schools have lost ground in terms of diversity and inclusion, thereby failing to achieve their social mission. 7 Nowhere is the social mission more critical than in the admissions process or entryway to health professions schools. Unfortunately, holistic admissions efforts may be misdirected, resulting in short-term gains in diversity statistics without fundamentally changing the institutional culture and local health outcomes. To achieve true health equity, medical schools and their affiliated health systems must commit to helping dismantle the structural impediments facing diverse learners and patients. Doing anything less makes them complicit in propagating the stark injustices of the US health care system.